

- History & Evolution
- Biosynthesis & dietary uptake
- UDCA and the microbiome
- UDCA and signaling
- UDCA as therapeutic drug
- UDCA and 5P medicine
- References
History & Evolution
1902: discovery in bear bile (Hammarsten) | 1927: isolation and naming (Shoda) | 1980s: approval for liver diseases
Ursodeoxycholic acid (UDCA) is a secondary bile acid with a long history in traditional medicine and modern hepatology. First identified in bear bile by Hammarsten in 1902 and isolated by Shoda in 1927, UDCA takes its name from Ursus, Latin for bear (Lazaridis et al. 2001). It became clinically relevant in the 1980s, when synthetic UDCA was approved for treating cholestatic liver diseases such as primary biliary cholangitis (PBC) (Ishizaki et al. 2005). Today, UDCA is recognized as a key therapeutic bile acid with a range of anti-apoptotic, cytoprotective and immunomodulatory functions (Lazaridis et al. 2001; Amaral et al. 2009).
Biosynthesis vs. dietary uptake
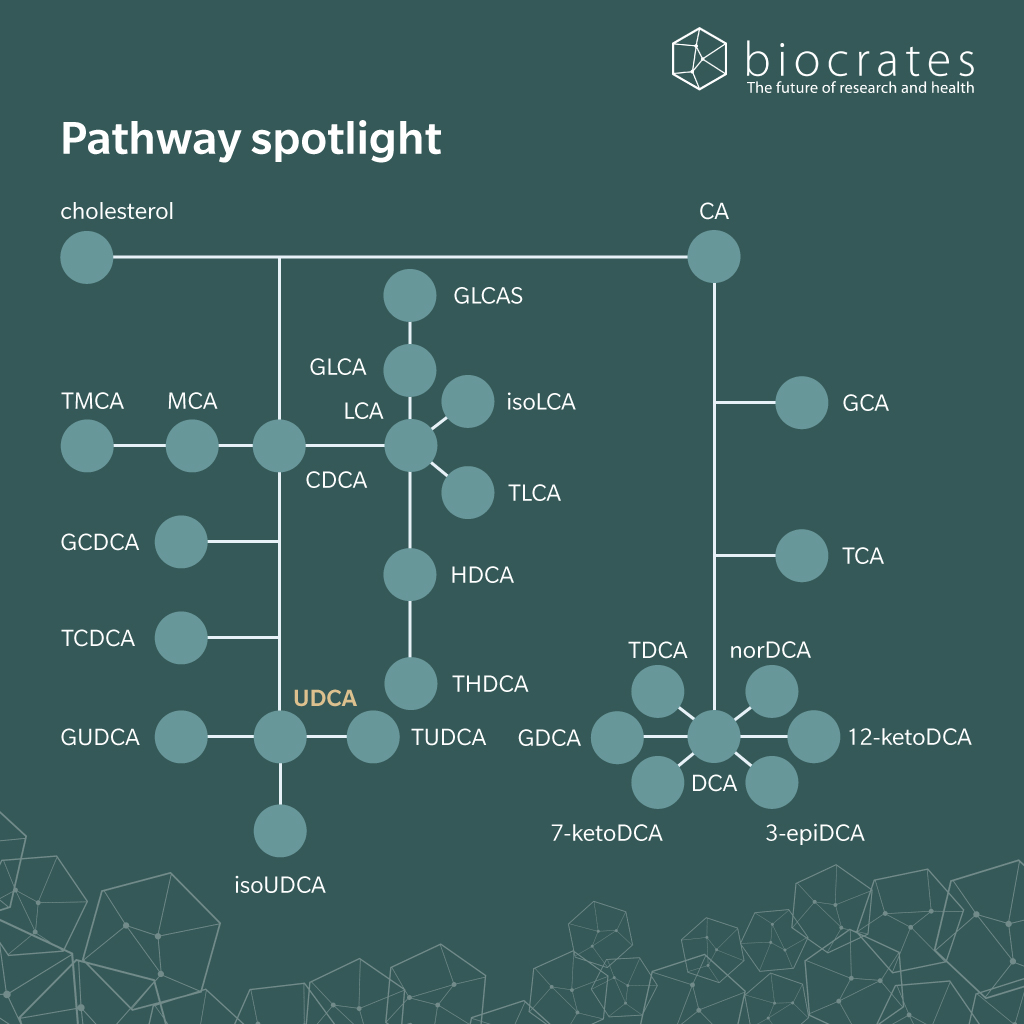
Bile acids are formed from cholesterol in the liver and secreted into the intestine. Gut microbiota metabolize these bile acids through deconjugation, dehydroxylation and epimerization (Keely et al. 2019). In this way, the secondary bile acid UDCA is produced in the colon through microbial transformation of the primary bile acid chenodeoxycholic acid (CDCA), first through deconjugation via bile salt hydrolases, then via epimerization at the 7-position (Daruich et al. 2019; Ridlon et al. 2015). Once formed, UDCA is passively absorbed in the colon and returns to the liver through the portal circulation. There, it is reconjugated with taurine or glycine into glyco- or tauro-ursodeoxycholic acid (GUDCA and TUDCA, respectively) as part of the enterohepatic circulation (Lazaridis et al. 2001). This recycling loop helps maintain bile acid pool stability and amplifies the systemic availability of UDCA. TUDCA and other conjugated forms of UDCA are increasingly recognized for their cytoprotective and anti-inflammatory properties (Daruich et al. 2019).
UDCA is not only a product of gut microbiota, but also a substrate for further transformation. The major metabolite of UDCA is lithocholic acid (LCA), which has been regarded as the most cytotoxic of the secondary bile acids, especially in the liver (Hofmann 2004). However, this view is increasingly being challenged. Emerging evidence suggests that the beneficial effects of UDCA on epithelial integrity and inflammation may, at least in part, depend on its microbial conversion to LCA (Lajczak-McGinley et al. 2020; Keely et al. 2019).
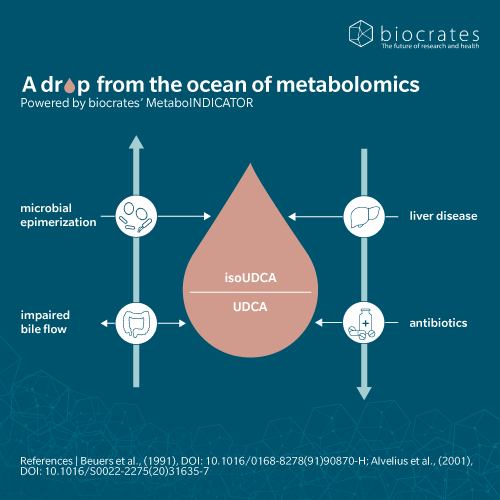
Additionally, UDCA can be reconverted into isoUDCA by microbial and hepatic enzymes. The ratio of isoUDCA to UDCA has been proposed as a potential biomarker of bile acid pool dynamics and therapeutic efficacy, particularly in cholestatic liver diseases (Beuers et al. 1991). This ratio reflects the delicate interplay between microbial metabolism and host bile acid handling; factors critical for maintaining bile acid homeostasis and preventing liver injury (Marschall et al. 2001).
UDCA and the microbiome
UDCA is both a product of microbial activity and a potent modulator of the gut microbiome itself. While its formation depends on bacterial enzymes, UDCA also feeds back into the intestinal environment, influencing microbial composition and function. This bidirectional relationship underlies many of UDCA’s therapeutic effects.
One of the key microbiome-level impacts of UDCA is its ability to shift microbial communities toward more balanced and less pro-inflammatory configurations (Wahlström et al. 2016). For instance, in experimental models of colitis, UDCA and its taurine-conjugated form TUDCA have been shown to normalize the Firmicutes-to-Bacteroidetes ratio, which can be indicative of microbial balance often disrupted in inflammatory and metabolic conditions. Such rebalancing may reflect reduced bile acid toxicity, improved mucosal barrier function, and downstream effects on immune regulation (Keely et al. 2019).
These microbiome changes are not only compositional but also functional. UDCA treatment is associated with a reduction in microbial pathways linked to harmful metabolites like enterobactin and lactate, while supporting bile acid transformations that favor anti-inflammatory and cytoprotective signaling (Lee et al. 2024).
Altogether, UDCA’s ability to modulate the microbiome reflects a broader mechanism of action that goes beyond its direct effects on bile flow or hepatocyte protection. Its role in shaping a gut ecosystem that supports intestinal and systemic homeostasis – an aspect of its therapeutic profile that is gaining increasing attention.
UDCA and signaling
In addition to its choleretic (promoting bile synthesis and bile flow) and cytoprotective effects, UDCA is increasingly recognized as a signaling molecule that modulates a range of nuclear- and membrane-bound receptors in human tissues (Marchianò et al. 2023). Although a relatively weak agonist compared to more hydrophobic bile acids like LCA or deoxycholic acid (DCA), which passively diffuse into epithelial colonic cells and activate nuclear receptors, UDCA exerts regulatory effects through both direct receptor engagement and indirect metabolic reshaping of the bile acid pool (Hanafi et al. 2018). These interactions contribute to UDCA’s therapeutic profile in liver and intestinal diseases (Lin et al. 2025).
Key receptor and signaling interactions
- Takeda G protein-coupled receptor 5 (TGR5, also known as GPBAR1): UDCA modestly activates this G-protein-coupled receptor, especially in enteroendocrine and immune cells. TGR5 activation enhances secretion of glucagon-like peptide-1 (GLP-1), supports glucose homeostasis, and suppresses pro-inflammatory cytokines such as tumor necrosis factor-alpha (TNF-α) (Hanafi et al. 2018), reinforcing UDCA’s metabolic and anti-inflammatory effects (Lin et al. 2025; Guzior et al. 2021).
- Farnesoid X Receptor (FXR): While UDCA is not a strong FXR agonist, it modulates FXR signaling indirectly by altering bile acid pool composition, notably by reducing antagonists like LCA (Hanafi et al. 2018). In inflammatory settings, UDCA can selectively downregulate FXR expression while upregulating FXR target genes like SHP, in turn influencing genes such as CYP7A1 and BSEP involved in bile acid synthesis and transport (Lin et al. 2025; Guzior et al. 2021).
- Pregnane X and Vitamin D Receptors (PXR and VDR): UDCA does not directly activate these receptors, but by reducing LCA – a potent ligand for both – it may help regulate detoxification pathways, epithelial integrity and immune homeostasis. These are especially relevant in gut-liver disorders and cholestasis (Hanafi et al. 2018; Keely et al. 2019).
There is also an epigenetic layer to UDCA’s anti-inflammatory and anti-tumorigenic mechanisms: UDCA downregulates miRNA-21, a pro-inflammatory and pro-carcinogenic microRNA that is upregulated by lipopolysaccharide (LPS) and in chronic liver inflammation (Peng et al. 2024).
UDCA as therapeutic drug
UDCA is a cornerstone therapy for chronic cholestatic liver diseases such as PBC, with growing relevance in metabolic and immunological conditions (Keely et al. 2019). While its core mechanisms are hepatoprotective and choleretic, UDCA also engages complex signaling and microbiome-modulating pathways that may benefit extrahepatic disorders like inflammatory bowel disease (Lin et al. 2025). As research evolves, combination therapies and system-level understanding will likely expand UDCA’s clinical applications across liver and gut health.
UDCA’s therapeutic effects stem from its ability to balance the bile acid pool, stabilize hepatocyte membranes, reduce oxidative stress and modulate immune responses (Kumar et al. 2001). These actions translate into anti-apoptotic, cytoprotective, choleretic and immunomodulatory benefits (Keely et al. 2019). In PBC, long-term UDCA therapy (13–15 mg/kg/day) improves liver biochemistry, slows histological progression and reduces the need for liver transplantation. It is most effective when started early and has become the standard of care (Kumar et al. 2001).
UDCA is also used in primary sclerosing cholangitis (PSC), though its benefits are modest and may be enhanced when combined with endoscopic therapy. It is the treatment of choice in intrahepatic cholestasis of pregnancy (ICP) and shows benefit in cystic fibrosis–associated liver disease, graft-versus-host disease, and pediatric cholestasis by reducing bile acid toxicity and supporting bile flow (Ted George O. Achufusi et al. 2023).
In metabolic dysfunction-associated steatohepatitis (MASH), UDCA alone has limited therapeutic efficacy but can enhance the effects of FXR/TGR5 agonists. Recent research showed that combining UDCA with such agents led to reversal of liver inflammation and fibrosis, improved bile acid signaling and greater metabolic gene regulation than either treatment alone (Marchianò et al. 2023). This positions UDCA as a synergistic component in multi-targeted approaches for metabolic liver diseases.
UDCA and 5P medicine
UDCA and its derivatives align well with all principles of 5P medicine:
- Predictive and personalized medicine: The isoUDCA/UDCA ratio has emerged as a potential biomarker for therapeutic response and bile acid pool dynamics in cholestatic liver diseases (Beuers et al. 1991). These profiles reflect microbial-host interactions and support individualized monitoring strategies (Marschall et al. 2001)
- Precision medicine: UDCA is an approved treatment for PBC, PSC and ICP (Kumar et al. 2001; Ted George O. Achufusi et al. 2023). It modulates bile acid receptors (FXR, TGR5), transporters and inflammatory responses (Hanafi et al. 2018; Keely et al. 2019). In MASH, UDCA is being tested in combination with receptor agonists like BAR502 (Marchianò et al. 2023). It also reshapes bile acid pools, reducing hepatotoxic intermediates such as LCA (Hanafi et al. 2018), thus acting as both a treatment and response-modifying agent.
- Participatory medicine: UDCA’s oral administration and safety profile allow patients to engage in long-term, proactive care. It is widely used to prevent gallstones in post-bariatric patients (Gideon M. Hirschfield et al. 2017) and treat pregnancy-related cholestasis (Kumar et al. 2001).
- Population-based medicine: UDCA is included in international clinical guidelines for PBC and other liver diseases (Lindor et al. 2019; Gideon M. Hirschfield et al. 2017). Its safety and efficacy support preventive use, although global access and cost remain variable.
References
Amaral, J.D. et al.: Bile acids: regulation of apoptosis by ursodeoxycholic acid (2009) Journal of Lipid Research | DOI: 10.1194/jlr.R900011-JLR200.
Beuers, U. et al.: Formation of iso-ursodeoxycholic acid during administration of ursodeoxycholic acid in man (1991) Journal of hepatology | DOI: 10.1016/0168-8278(91)90870-H.
Daruich, A. et al.: Review: The bile acids urso- and tauroursodeoxycholic acid as neuroprotective therapies in retinal disease (2019) Molecular Vision | PMID: 31700226
Gideon M. Hirschfield et al.: EASL Clinical Practice Guidelines: The diagnosis and management of patients with primary biliary cholangitis (2017) Journal of Hepatology | DOI: 10.1016/j.jhep.2017.03.022.
Guzior, D.V. et al.: Review: microbial transformations of human bile acids (2021) Microbiome | DOI: 10.1186/s40168-021-01101-1.
Hanafi, N.I. et al.: Overview of Bile Acids Signaling and Perspective on the Signal of Ursodeoxycholic Acid, the Most Hydrophilic Bile Acid, in the Heart (2018) Biomolecules | DOI: 10.3390/biom8040159.
Hofmann, A.F.: Detoxification of lithocholic acid, a toxic bile acid: relevance to drug hepatotoxicity (2004) Drug metabolism reviews | DOI: 10.1081/dmr-200033475.
Ishizaki, K. et al.: Hepatoprotective bile acid ‘ursodeoxycholic acid (UDCA)’ Property and difference as bile acids (2005) Hepatology Research | DOI: 10.1016/j.hepres.2005.09.029.
Keely, S.J. et al.: Ursodeoxycholic acid: a promising therapeutic target for inflammatory bowel diseases? (2019) American journal of physiology. Gastrointestinal and liver physiology | DOI: 10.1152/ajpgi.00163.2019.
Kumar, D. et al.: Use of ursodeoxycholic acid in liver diseases (2001) Journal of Gastroenterology and Hepatology | DOI: 10.1046/j.1440-1746.2001.02376.x.
Lajczak-McGinley, N.K. et al.: The secondary bile acids, ursodeoxycholic acid and lithocholic acid, protect against intestinal inflammation by inhibition of epithelial apoptosis (2020) Physiological Reports | DOI: 10.14814/phy2.14456.
Lazaridis, K.N. et al.: Ursodeoxycholic acid ‘mechanisms of action and clinical use in hepatobiliary disorders’ (2001) Journal of hepatology | DOI: 10.1016/S0168-8278(01)00092-7.
Lee, J. et al.: The gut microbiome predicts response to UDCA/CDCA treatment in gallstone patients: comparison of responders and non-responders (2024) Scientific Reports | DOI: 10.1038/s41598-024-53173-2.
Lin, X. et al.: Crosstalk Between Bile Acids and Intestinal Epithelium: Multidimensional Roles of Farnesoid X Receptor and Takeda G Protein Receptor 5 (2025) International Journal of Molecular Sciences | DOI: 10.3390/ijms26094240.
Lindor, K.D. et al.: Primary Biliary Cholangitis: 2018 Practice Guidance from the American Association for the Study of Liver Diseases (2019) Hepatology | DOI: 10.1002/hep.30145.
Marchianò, S. et al.: Combinatorial therapy with BAR502 and UDCA resets FXR and GPBAR1 signaling and reverses liver histopathology in a model of NASH (2023) Scientific Reports | DOI: 10.1038/s41598-023-28647-4.
Marschall, H.-U. et al.: Isoursodeoxycholic acid: metabolism and therapeutic effects in primary biliary cirrhosis (2001) Journal of lipid research | DOI: 10.1016/S0022-2275(20)31635-7.
Peng, C.-Y. et al.: Ursodeoxycholic Acid Modulates the Interaction of miR-21 and Farnesoid X Receptor and NF-κB Signaling (2024) Biomedicines | DOI: 10.3390/biomedicines12061236.
Ridlon, J.M. et al.: The human gut sterolbiome: bile acid-microbiome endocrine aspects and therapeutics (2015) Acta pharmaceutica Sinica. B | DOI: 10.1016/j.apsb.2015.01.006.
Ted George O. Achufusi et al.: Ursodeoxycholic Acid (2023) | PMID: 31424887
Wahlström, A. et al.: Intestinal Crosstalk between Bile Acids and Microbiota and Its Impact on Host Metabolism (2016) Cell Metabolism | DOI: 10.1016/j.cmet.2016.05.005.